

Naming convention of the DMN lateral regions
Hi,
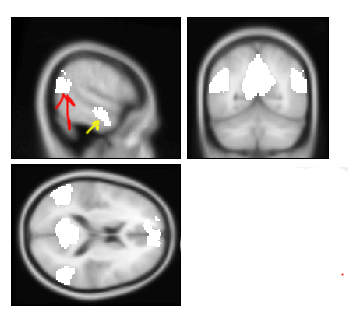
There are two well-known lateral posterior-temporal regions (red and yellow arrows). The posterior one (red arrow) is mostly at the area of Angular gyrus, however it also encompasses some portions of the posterior superior temporal gyrus and posterior middle temporal gyrus. The anterior one (yellow one) encompasses mostly anterior superior temporal gyrus and inferior temporal gyrus . In my paper I need to name somehow this posterior STG/MTG cluster and this anterior STG/ITG region. How you suggest I avoid the confusion for the paper reader, given that previous literature sometimes name the anterior region MTG or STG.
Thanks a lot,
Vadim
ddburman
Wed, 12/04/2013 - 16:59
Permalink
Re: Naming convention of the DMN lateral regions
I would name the regions as angular gyrus and anterior MTG, which aptly describes the largest regions affected. The posterior region in the dominant hemisphere looks like Wernicke's area, sometimes described as posterior MTG in studies of semantics / comprehension. (The anterior region is also sometimes activated in semantic studies.)
axel.vadim
Wed, 12/04/2013 - 20:07
Permalink
Thank you, Doug. Then I will
Thank you, Doug. Then I will probably name them pSTG and aSTG.
You are right regarding the pSTG - it was indeed selective to language processing.
BTW, do you also see the pSTG as part of DMN activation? In my case the seed was in the PCC. People usually refer to this large posterior lateral blob as angylar gyrys / IPS, so I wondered whether it's a usual practice to get also the pSTG there.
find37
Wed, 12/04/2013 - 21:18
Permalink
Hi Vadim,
Hi Vadim,
Best to use an anatomical reference that best describes that region (peak coordinates are commonly used for this). The angular gyrus is the more typical lateral parietal portion of the DMN (depending on methods used- notably on seed placement in seed-based methods). Here are the results from a PCC seed from task-free data in 892 older cognitively normal subjects. The lateral parietal region seen here is best characterized by the angular gyrus (I suspect yours is as well). Anatomical landmarks for lobes, brodmann areas, etc can be helpful and depending on the platforms you are using there are packages to help you label the anatomic sites of interest.
Best,
Dave Jones
axel.vadim
Wed, 12/04/2013 - 21:45
Permalink
Thank you Dave.
Thank you Dave.
Sure, large portion of the posterior lateral blob is the AG is in my data as well. pSTG is in addition.
BTW, I get relativley weak activations in the ventral ACC (compared to BA 10, for example). With 892 subjects the power should be higher, I guess...
find37
Wed, 12/04/2013 - 23:34
Permalink
I don’t find any ACC using
I don’t find any ACC using the PCC seed based analysis I showed either…. So these analyses would be in agreement despite any power differences. However, move the seed, change the dimensionality of an ICA analysis, or have a population with greater ACC involvement in MPFC and PCC based brain configurations and you will find ACC involvement with “DMN regions.”
Best,
Dave
find37
Wed, 12/04/2013 - 23:47
Permalink
That being said, with
That being said, with increased power I can more confidently lower the threshold and then I do see the vACC and medial temporal lobe contributions.
axel.vadim
Thu, 12/05/2013 - 09:14
Permalink
thnaks, this is useful for me
thnaks, this is useful for me to know
ZangYF
Thu, 12/05/2013 - 05:30
Permalink
RE: [RFMRI] Naming convention
For the anatomical naming convention, I just have additional
suggestion. Sometime the naming varies a lot from study to study. I’d like to
suggest provide more information, e.g., anatomical name (with the reference
tools would be better), BA, and peak coordinates.
Yufeng
From: RFMRI.ORG
[mailto:rfmri.org-bounces@rnet.co] On Behalf Of The R-fMRI Network
Sent: Thursday, December 05, 2013 7:35 AM
To: rfmri.org@rnet.co
Subject: Re: [RFMRI] Naming convention of the DMN lateral regions
[To post a comment, please reply to
rfmri.org@gmail.com ABOVE this line]
Commented by David Jones (find37)
I don’t find any ACC using the PCC seed based analysis I
showed either…. So these analyses would be in agreement despite any power
differences. However, move the seed, change the dimensionality of an ICA
analysis, or have a population with greater ACC involvement in MPFC and PCC
based brain configurations and you will find ACC involvement with “DMN
regions.”
Best,
Dave
Online version of this post:
To manage subscriptions, please visit:
Mail comment ID:
axel.vadim
Thu, 12/05/2013 - 09:16
Permalink
thank you
thank you
I plan to provide anyway coordinates list of my ROIs
ddburman
Fri, 12/06/2013 - 15:00
Permalink
RE: [RFMRI] Naming convention
I would agree with the later comments that it is best to refer to the region by the anatomical reference, including all the areas in a table that specifies maxima coordinates, etc.
How much angular vs. posterior middle (& superior) temporal gyrus is activated by language depends on the particular task, individual(s), and study. Part of the DMN is more active during demanding language conditions, e.g., requiring conversion of information between visual & auditory modalities – which seems to contradict the idea that the DMN is most active when we are doing nothing.
Personally, I think the DMN is involved in associative activity, so that by default we make associations between whatever stimuli and/or thoughts that occur simultaneously in time – there is decreased activity when we are doing a task so that irrelevant information does not interfere or create dysfunctional associations. This hypothesis explains why demanding tasks [which nearly always require associations] are associated with more activity in the DMN than less demanding tasks, although not as much overall as at rest. Furthermore, it explains the symptoms with neurological conditions such as Alzheimer’s that are associated with lower DMN activity – reduced ability to form new (associative) memories and loss of other abilities that require associative references (such as spatial navigation and math).
Doug Burman
Legal Disclaimer: Information
contained in this e-mail, including any files transmitted with it, may contain
confidential medical or business information intended only for use by the
intended recipient(s). Any unauthorized disclosure, use, copying,
distribution or taking of any action based on the contents of this email is
strictly prohibited. Review by any individual other than the intended
recipient does not waive or surrender the physician-patient privilege or any
other legal rights. If you received this e-mail in error, please delete it
immediately and notify the sender by return email.